Note: While the skills covered in this article can help save lives, you must attend first-aid training classes such as those offered through the American Red Cross prior to attempting them.
“The fate of the wounded rests with the one who applies the first dressing.” - Nicholas Senn
The past 15 years have seen a marked shift in the focus of emergency medical care. Tourniquets are no longer bad things, the ABCs aren’t always followed in that order, the efficacy of advanced life support for trauma has been questioned and even supplemental oxygen may be bad for some people.
But one thing that hasn’t changed is the fundamental precept of emergency medical care: blood goes ‘round and ‘round, air goes in and out and any variation on this theme is a problem.
Quite often, the correction of those variations is time-sensitive. So time-sensitive, in fact, that if you wait until professional help arrives, the patient may be beyond help. Recognition of the importance of prompt intervention and self-care is what spurred the US Army to develop the Combat Lifesaver designation, in which a non-medic soldier trained in rudimentary lifesaving skills can help keep another soldier—or himself—alive until the combat medic arrives.
There are plenty of first-aid courses available out there, and if you have the time and resources, I’d encourage you to take one. An Emergency Medical Responder course will take upward of 48 hours of classroom time and skills practice to complete, and will teach you the basic skills and knowledge to handle all manner of medical and traumatic emergencies with confidence, at least until more capable help arrives. Many of the trauma-care training courses you see online are based upon Tactical Combat Casualty Care, which is a combat-oriented version of Prehospital Trauma Life Support. Such courses offer a wealth of training and information, but they are geared toward specialty certification of Emergency Medical Technicians and Paramedics, and the level of training is well over the head of the average layperson.
The blowout kit
Much like the first rule of a gunfight is to bring a gun, the first rule of medical emergencies is to bring medical supplies. A personal blowout kit such as this one is small enough to fit on a belt or in a range bag. The addition of a tactical tourniquet and a package of adhesive chest seals will provide you with all the essential lifesaving gear you need for the first few minutes of an emergency, for less than $100.

Get good supplies, and learn to use them properly. While a medical expert may be able to fashion a tourniquet out of a Bic pen and three stale pieces of licorice, a layperson doesn’t need to handicap himself further with improvised equipment.
It may come as a surprise to you, but medical professionals are every bit as susceptible to "derpitude" as shooters. If you wouldn’t fall for buying some boutique bullet that claims to instantly stop a meth-fueled psychopath with a chest wound resembling a burping, smoking geyser, don’t fall for buying some useless wound clamp or handy-dandy, bandage-injecting turkey baster, either. Those things are designed to separate fools from their money, not save lives.
Likewise, avoid using improvised trauma dressings such as sanitary napkins or tampons. They are not designed to stop large amounts of bleeding. Most of us don’t use cheap ammo or a shoddy holster to secure our carry weapons, and for good reason. The same philosophy holds for saving your life; this is not a time to improvise a dressing when there are inexpensive, readily available products that work better.
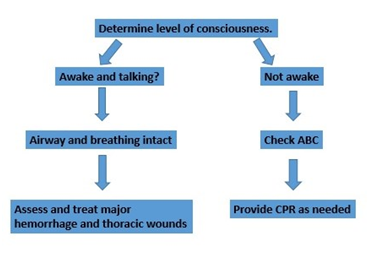
The primary survey
The first step in providing lifesaving care is to identify threats to airway, breathing and circulation. This assessment and intervention process is called the primary survey, and everything you’re looking for is what will kill the patient in the next few minutes, and needs to be fixed right now.
Simply put, if the victim is able to talk and can tell you where he’s hurt, his airway is open and his breathing is adequate. All you have to do is find and plug the holes. Strip the area in question down to bare skin and observe the wound. Aside from massive damage to the central nervous system – which we are unable to do much to stabilize – arterial bleeding and thoracic wounds are the most likely to kill quickly.
Open pneumothorax
A hole in the chest making a sucking noise and bleeding pink, frothy blood is an open pneumothorax, ie the proverbial “sucking chest wound.” Such wounds should be managed immediately. Managing it is as easy as “peel ‘n stick.” Open your adhesive occlusive dressing, such as the HALO Seal or Asherman Chest Seal, and stick it to the wound. The one-way valve in the chest seal will prevent atmospheric air from being sucked into the wound, yet still allow air leaking from the damaged lung to escape, helping prevent its total collapse.
However, sucking chest wounds are not nearly as common as you might think. To entrain air, a hole in the chest needs to be quite large, at least 2/3 the diameter of the trachea. Rifles, knives, and shotguns at close range are capable of producing such wounds, but pistol caliber rounds tend to poke small, innocuous-holes in elastic flesh. The real danger comes from the damage you can’t see.
Arterial bleeding
It sounds incongruous to say this, but armed combat has never been as survivable as it is today, at least for U.S. armed services members. Part of that is due to the training and equipment we provide them, but the larger part is due to the military’s recognition of the most common treatable cause of combat death—uncontrolled extremity hemorrhage. And that has spurred the resurgence of the arterial tourniquet, in a big way.
Tourniquets had been considered the bleeding control treatment of last resort for a generation or more, based upon dogma, flawed supposition, and anecdote dating as far back as the Crimean War. The old treatment sequence of direct pressure, elevation and manual compression of arterial pressure points simply allowed the patient to bleed to death a little more slowly than before. If the wars in Iraq and Afghanistan have taught us one thing, it is that the negative consequences of tourniquet use are manageable…if the patient makes it to surgery alive. Simply put, tourniquets make that much more likely to happen.
You’ve got 30-60 seconds to apply the tourniquet. Most combat tourniquets are designed to be applied with one hand, and which one works best is mainly a matter of personal preference. The SOF-TT and the CAT tourniquet are two popular choices. Apply the tourniquet about six inches proximal to the bleeding site, secure in place, crank the windlass until the bleeding is stopped, and lock the windlass in place per manufacturer’s instructions. Heavy clothing and bulky items like rifle magazines in cargo pockets interfere with arterial compression, and skeletal joints are non-compressible anyway, so avoid placing the tourniquet over those. Fair warning, though: tourniquets hurt, quite a bit.
But in the words of that noted philosopher Shane Falco, “Pain heals. Chicks dig scars. Glory… lasts forever.”
One item that makes a useful adjunct to a tourniquet, is a hemostatic dressing designed to speed clotting. Most of these dressings are infused with a hydrophilic clay or mineral compound, or a protein matrix made from chitosan, a byproduct of shrimp shells. Chitosan is safe even for those people with shellfish allergies. Hemostatic dressings got a bad rap in their early years for their difficulty in use, high price, and tendency to cause burns and other complications. However, as formulations and techniques have been refined, they have proven quite useful. They won’t stop arterial bleeding by themselves, but they will help make up for flaws in your wound care technique. Shop around for one that fits your budget, and use it according to manufacturer’s directions.
Cardiopulmonary resuscitation
Only two interventions are scientifically proven to be effective in the treatment of sudden cardiac arrest; prompt defibrillation, and continuous, high quality chest compressions. Everything else is just theory, and of questionable benefit – and that includes everything I do as a paramedic. Simply put, if the victim has not received quality CPR and adequate defibrillation, all the Advanced Life Support in the world is pointless.

If the victim appears unconscious and not breathing, place the heels of your hands squarely between the nipples, and compress the chest roughly two inches, 100 times per minute. There are CPR metronome apps for your smartphone, or you can just sing “Stayin’ Alive” to yourself to keep your rhythm.
Rescue breathing, at least provided by the layperson rescuer, is not necessary. Research shows little benefit to rescue breathing in sudden cardiac arrest, and for reasons too complicated to explain here, it may even hinder your chances of a successful resuscitation.
There is no need to check for a pulse, either. Most laypeople do a poor job of at detecting a pulse, particularly under the stress of a resuscitation. For your purposes, unconsciousness + lack of breathing = chest compressions. If the victim opens his eyes and pushes your hands away, stop doing compressions, but otherwise keep going until the paramedics arrive.
Treating shock
The best way to treat shock is to prevent it. Prompt control of arterial bleeding and management of chest wounds is essential. Once those things are done, lie the victim down and cover with a blanket. There is no need to raise the legs, and if the arterial bleed is in one of the legs, moving them around may break open clots and renew bleeding. There are other things we can do to treat shock, but they are beyond the capability of the layperson.
Summary
Often, the most important and time-critical lifesaving interventions are the most simple to apply. These interventions are the same that a trained rescuer would do in the first few minutes, and are well within the capabilities of a layperson. An article in Shooting Illustrated and a few YouTube videos are no substitute for a formal trauma care course, but at least these tips may give you the tools to save your own life, and the confidence to do something more for your shooting buddy than stand around helplessly until the ambulance arrives.
Safe shooting, everyone!